
How GLP-1s are transforming binge eating and big food

A staggering one in eight Americans has tried GLP-1s. We know that, in addition to weight loss, they also help reduce the risk of conditions like type 2 diabetes and cardiovascular disease, and have a role in preventing neurodegenerative diseases like Alzheimer’s or Parkinson’s. But GLP-1 use impacts a common and less discussed condition—binge eating. And the effects are transforming big food.
As a former food entrepreneur, I know more than I wish I did about that profoundly flawed system. I’ve followed it closely for over a decade, and believe that its moment of reckoning is finally here, and not for the reasons I expected.
The genesis of this piece came from conversations with Emilie Faure, founder and CEO of Juniver, an eating disorder company, about the interconnection of binge eating, GLP-1s, and our food system. Here is what we wish everyone knew.
Binge eating is incredibly common
When most people think of disordered eating, anorexia—a condition characterized by undereating and overexercising—is the first thing they think of. But binge eating disorder (BED) affects nearly 3 percent of the U.S. population—more than double the reported numbers for bulimia nervosa and anorexia. Unsurprisingly, prevalence is around 2x more likely in women than men. Obesity is one comorbidity for binge eaters, but not always, and the condition is often missed.
Juniver’s Emilie Faure shared with me, “GLP-1s are promising for binge eating disorder, curbing urges and quieting food noise, but medication alone isn’t enough. For recovery to stick, patients need real wrap-around solutions with community support, behavioral coaching, and digital tools that are always on and flex to symptoms. Especially as we know that people are cycling on and off GLP-1s because of changes in coverage or side effects, which is affecting the medications’ efficacy. Support during transition phases and solutions tailored to people with binge-eating disorder is what we’re building at Juniver.”
So what causes binge eating? The answer is, it’s complicated and multifactorial. However, research indicates that BED patients who report bingeing did so on 100% of ultraprocessed foods, which are high in fats and carbohydrates and low in protein. When given the choice between cocaine and sugar, lab rats go straight for the sweet stuff too. Cravings for ultraprocessed foods light up the same part of the brain as addiction, and provoke compulsive behavior. If GLP-1s drive down demand for these foods, we may see less on grocery store shelves that inspires binge eating.
This may already be happening. A recent study showed that households with at least one GLP-1 user reduced their grocery spending by 6% after starting treatment; higher-income households reduced their spending by 9%. These reductions were mainly on calorie-dense, processed foods and savory snacks, which saw an 11% decline. Snack foods have long been seen as a growth driver in the food industry. But now, consumers are moving more toward healthier snacks and mini-meals, which are also better suited to GLP-1 users. This shift is having financial consequences for big food, with PepsiCo’s Frito-Lay brand reporting a 3% loss in sales volume last quarter. Last quarter, General Mills snack sales fell 5%, and JM Smucker’s sweet-baked snacks sales fell 7%.
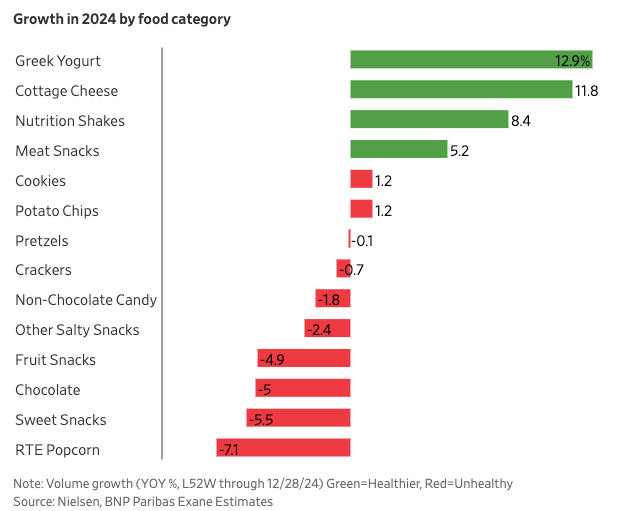
Source: WSJ, Snack sales in 2024
While the recent so-called snacking showdown is attributed to inflation and increased food costs, the long-term effect of GLP-1 adoption will be permanent. Combined with consumer enthusiasm for better options and the increased desire to eat at home and prepare healthier meals post-COVID, we expect to see deeper interrogation of how we make food in the first place. For example, “minimally processed” is a trend and product characteristic that drives growth for frozen food.
Manufacturers like Conagra are reformulating and labeling foods specifically to appeal to GLP-1 users, doubling down on nutrient-dense purchases like yogurts and produce. We also expect the “farm to table” trend to grow, as it hits on what’s happening in government, and resulting products will be better suited to the many GLP-1 users. Foods on shelves are getting labels that indicate their suitability to GLP-1 users. One example is Conagra’s “On Track” badge on Healthy Choice products, which means they are formulated with GLP-1 users' nutritional needs (like higher protein) in mind.

How GLP-1s reduce binge eating
GLP-1s reduce “food noise,” aka persistent thoughts a person has about food, regardless of hunger. Exactly how this happens isn’t fully understood. GLP-1s seem to affect the dopamine systems, and emerging evidence points to GLP‐1 receptors as a possible target for developing new pharmacological treatment options for addiction across food, alcohol, gambling, and other compulsive behaviors.
Silencing a binge eater’s food voices with GLP-1s is a great start. But as Dr. Priya Jaisinghani, a New York-based obesity doctor, told us, “For patients living with BED, treatment works best when it is comprehensive. That means addressing the psychological, behavioral, and metabolic aspects together. Since BED is a complex condition that affects both the body and mind, treatment decisions should always be tailored to the individual.”
On that note, GLP-1s use has a less positive effect for those struggling with disordered eating, too: reviving diet culture and an idealization of thinness. This shift betrays the hope for a different reality fostered by body positivity movements and their celebrity advocates, and ultimately, may increase the risk of disordered eating behaviors. The psychological aspects make holistic care that meets people where they are, while triggered, critical.
There is also a significant behavioral and community support gap left by GLP-1 prescriptions, which limits patients’ ability to build sustainable recovery beyond medication. This aspect of treatment is missed because many providers prescribing GLP-1s have inadequate (or zero) real training in managing eating disorders.
We want to acknowledge that GLP-1s are not FDA-approved (yet) for BED treatment. Many unanswered research questions exist, especially about how they affect different body compositions, races, and ethnicities, and their long-term safety in this population. GLP-1 users and people with eating disorders are predominantly women, and almost all pre-clinical studies in these areas were conducted on male animals.
Even if indicated for another condition like obesity, GLP-1s are no silver bullet for everyone. As we see more research about their positive impacts, we also know that many people stop taking them within a year because of various factors, including the cost and the side effects.
Dr Laura Berner, Associate Professor of Psychiatry and Director of the Neuroscience of Eating and Associated Pathology Research Program at Mount Sinai and advisor to Juniver emphasizes "The reduction in binge eating and related thoughts seen in some of these studies and in anecdotal reports support what rodent research has suggested for years: that GLP-1 receptors could play a key role in BED symptoms. That said, the goal of treatment for BED is not to indiscriminately reduce all eating, but to specifically decrease binge eating. These medications may help, but more research is needed, and most prescribers are not adequately trained to assess, monitor, or treat eating disorder symptoms."
Quieter food voices = less binge-worthy snacks
Even without an official indication, GLP-1s are still making it into the hands of many BED patients with comorbidities that are approved for their use. Without the constant drumbeat of their food voices, binge eaters taking GLP-1s eat less, and what they want to eat changes too. GLP-1s slow gastric emptying, which can cause nausea when someone overeats, reducing the amount of food consumed. This is causing an unexpected effect for GLP-1 users: their taste and texture preferences change from highly processed foods toward fresh foods.
Bingeing on ultra-processed foods may become less appealing in the future. Sixty percent of the American food supply is ultra-processed foods. These ultra-processed “hyper-palatable” foods, which help drive obesity, aren’t as tasty to people on GLP-1s, prompting big food to rethink its formulas. These drugs could, in effect, weaken the desire for the carefully engineered flavor and texture profiles that fuel binge eating.
Big food is due a reckoning—we’re glad it’s happening, for ourselves and the world we want for the next generation, i.e., our kids. I was so passionate about this mission that I started a company in the alternative protein space nearly a decade ago called Bitty Foods. What was true then and is still true now is that processed foods are not what they should be, and many are explicitly formulated to stoke a vicious cycle of addictive binge eating.
Where are we headed from here?
GLP-1s are incredible drugs, and great tools for binge eating, but not a perfect solution in isolation. They curb compulsive eating, but issues with side effects and cost/coverage mean that people will likely take them for limited periods. True long-term success in treating binge eating requires wrap-around support: ongoing therapy, nutritional guidance, peer/community support, and monitoring. Combining medication with well-rounded care makes it possible to quiet “food noise” and build sustainable, healthy habits that endure long after any prescription ends. Also, we need more research, as GLP-1s have different effects on women.
Even if GLP-1s were fully approved for BED treatment, insurance coverage is declining in 2025, so cost is a significant barrier for patients even with discounts. Employers, payers, and regulators are under growing pressure to ease access to anti-obesity and anti-addiction medication, especially with a broader spotlight on how diet and metabolic factors contribute to public health crises.
Now that the name-brand shortage is over, online GLP-1 compounding pharmacies are in limbo. Eli Lilly now sells Zepbound directly for $349/month, and it’s available via telehealth on Ro and Hims & Hers. Novo Nordisk is offering Wegovy directly for $499/month too. We expect more direct deals, especially as new versions launch. But in the meantime, without coverage and even at a discounted rate, the cost still puts it out of reach for many people who want or need it. This makes other treatment options like CBT and health startups working on this problem crucial to curb binge eating.
Consumers are voting with their wallets when it comes to what they eat, and there appears to be political will in DC to make meaningful changes to the food system at the federal level. Ultimately, the hope is that this virtuous cycle of reducing the number of binge-worthy snacks on shelves leads to a world where fewer people need GLP-1s for long periods or at all, and we see the number of BED patients decline as well. But until then, it’s all hands on deck, and we need smart people working on this problem.
This is part of a series exploring the unintended consequences of GLP-1s. What do you think should be next? Send me a note: leslie@secondopinion.media
About the author